Lower A1C Report: 3 Questions Your Doctor Wishes You’d Ask
Congratulations. We’ll see how long it lasts.
That’s such a pessimistic view and maybe even passive aggressive, isn’t it?
Out loud, I never finish that sentence beyond congratulations.
And yet, whenever I see a patient come in with a huge drop in their A1C and they’re super excited, or whenever I see someone post a dramatic drop online that they’re really proud of, I kind of worry and I think we’ll see how long that lasts.
And I do feel guilty about thinking that way because who am I to potentially spoil their accomplishment?
I gave the generic response. I said, “Congratulations. Well done. Keep up the good work.”
And it is good work and it deserves to be celebrated.
Honestly though, I knew their work wasn’t done yet.
I know something that nobody said out loud, that the A1C is not the finish line.
This moment might actually be the most dangerous moment in the diabetes journey.
And I didn’t want that person to get complacent.
Why is that?
Because for most people, this moment creates a crucial shift in thinking.
They think to themselves, “Oh yeah, I’ve got this all figured out.”
So they stop asking questions. They stop being vigilant and they start letting things slide.
And other people think they’re so lucky because they might have given up hope and silently ask themselves, “Why couldn’t I have that success? Why couldn’t I be cured? Why do I have to live with this disease and let it dictate my life when I go out with family and friends?”
So today I want to give you the three questions your doctor wishes you would ask when you get a great report card and how the answers to these questions can shift your perspective to lead towards lasting change.
Question 1: Is this true remission or just improved control?
A lot of people walk in the clinic, they see a better A1C and they are super excited.
Usually whenever the doctor tells them about the new result, they’re just wide-eyed and they say, “Oh, wow!”
And their eyes light up because they accomplished such an amazing feat.
And they think they have it all figured out and that they’ll keep doing what they’re doing.
But maybe reward themselves more frequently because they think that they can just buckle down when necessary in order to do it again.
And they don’t realize that it may be harder the next time around.
But many people don’t realize that the work is just beginning.
There needs to be a greater self-awareness.
Knowing the difference between true remission and just improved control matters more than just a good A1C result.
So what is that difference?
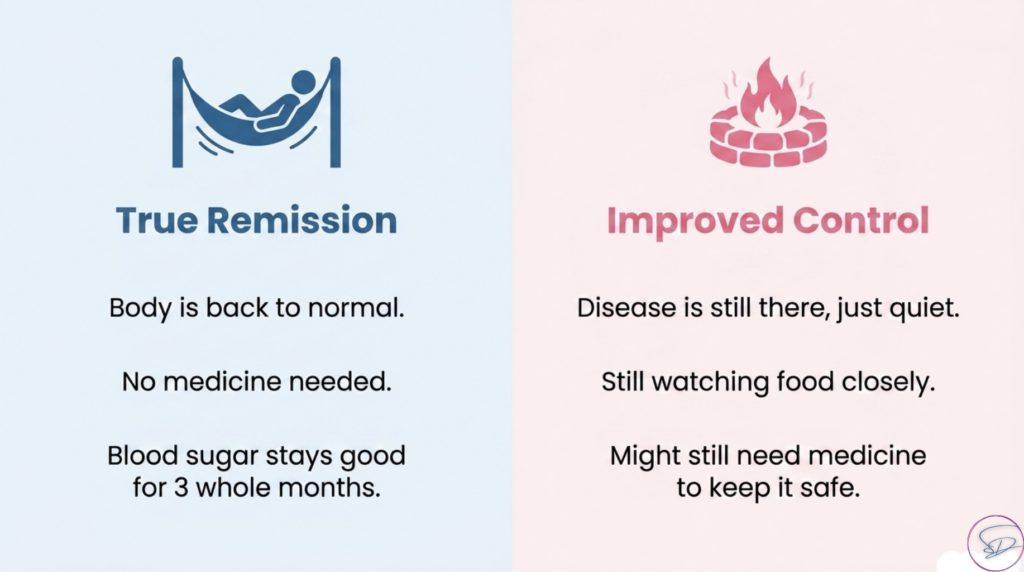
True remission means your body is back to normal.
Your body is not in a state of diabetes.
So you don’t have to:
- Obsess over every meal.
- You don’t need medication.
- And most importantly, the underlying physiology of diabetes is no longer active in the body.
Versus improved control would mean that the disease is still there.
- It’s just quieter.
- You still have to watch what you eat.
- You may still need medication or need to restart it down the road.
So, we basically controlled the fire, but you can still easily burn yourself without taking proper precautions.
So, how do you tell the difference? How do you know what state you’re in?
How do you tell the difference if you’re in true remission or improved control?
The honest answer is that you have to listen to your body.
The only way to know if you’re controlled or in remission or even relapsing is to pay attention to what your body is telling you.
What is the feedback?
- We do this by checking the A1C.
- We do this by seeing how your blood sugars respond to medication, to different foods.
If your blood sugar goes up, we adjust. If your blood sugar goes down, we adjust again.
So, it’s a process of careful supervised trial and error and watching how your blood sugar responds.
If your levels stay normal without any medication for 3 to 4 months, that’s when we can start talking about remission.
But here’s what you need to understand: The body remembers.
If you think about building muscle, the first time you do it, it’s really hard.
You have to really work hard to build it up and get the gains that you’re looking for.
But let’s say you stop for a period of time, the muscle will fade over time.
But when you go back to the gym and you hit those weights again, the muscle seems to come back faster than it did before.
Body remembers how to rebuild that muscle even if it hasn’t been there in a long time.
Diabetes seems to work in the same way.
Even though your body might have diabetes in a state of remission, your body can find its way back to a diabetic state much more easily than it got there the first time.
So the answer to question one is: Are you paying attention to your body’s new balance?
With a focus on how to adjust the scale rather than what the scale actually says, you start to ask the questions that can tip the scale in your favor.
So, for example,
- Can we wean off any medications? If so, which ones and how fast?
- Should I check my sugars before I eat or after I eat?
- Should I use a CGM device to monitor the progress?
- Do I still need the usual checks for my eyes and feet and blood pressure and kidneys? And if so, how often do I need to check them?
Because as we’re checking these things, we’re asking the second question now.
Question 2: How do we prevent relapse?
It seems to me that a lot of people think if you relapse, you gave up.
As if you decided to just stop trying one day.
But that’s almost never how it happens.
Relapse is quiet.
It’s gradual.
It slides in.
It’s kind of creepy.
It starts even before your A1C moves up.
It shows up a little at a time.
- You got a little weight creeping back on
- A few nights of bad sleep
- A new medication that your doctor might have prescribed
- that nobody told you that it affects your blood sugar
- Or maybe you have sleep apnea,
- which most people never even really connect to diabetes because their doctor only ever might mention it in relation to blood pressure.
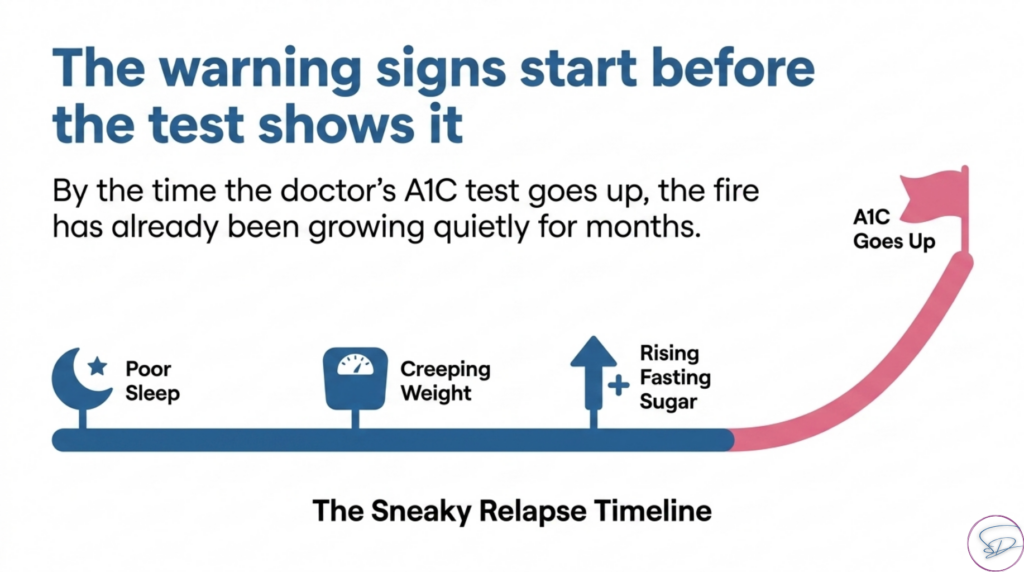
So by the time the A1C flag goes up, the process has already been happening for months.
So the warning signs to watch for aren’t as dramatic as the latest telenovella episode.
They’re quieter than that.
They’re more gradual than that.
- They’re a rising fasting blood sugar level.
- They’re slightly worse sleep or not feeling so good when you wake up in the morning.
- They’re a couple extra inches on the waistline.
So, those are some of the early warning signs.
But here’s what nobody talks about:
The real reason people relapse isn’t because they magically forgot what to do.
It’s not because of diet and exercise and medication that somehow magically stopped working or helping.
It’s because the habits that might hurt people are also serving them.
So, they creep back into daily life.
- The ice cream before bed isn’t always an indulgence. It’s how someone spends quality time with their family.
- Sitting after dinner and watching TV isn’t laziness. It’s exhaustion from working a full day to pay the bills.
- Financial security for their family matters.
- Comfort food isn’t a weakness. It’s how someone might survive a divorce.
After the doctor tells the patient what not to eat anymore or to cut back on, the patient finally asks, “But doc, what’s left to eat?”
And as far as I can tell, what they’re really asking underneath that question is, “Why are you taking away everything that makes life worth living?”
And that’s a hard question because it’s not really about food at all.
I get the sense that there is a fear of grief in that question because they’re giving something up.
They’re losing something that matters to them in their life.
So instead of telling you what to give up, I want to ask you:
- What does your food actually mean to you?
- What would you miss?
- What would you grieve?
- What does it really represent?
Because once you can face these questions, you can start building a life that protects both your health and the things that make life worth living.
So ask your doctor three things:
- Am I actually in remission or just well controlled?
- Second, what is my relapse monitoring plan?
- And what number should make me call you and come back into the office?
- And then third, could something silent be pushing my blood sugars back up?
- Something like sleep apnea which can worsen insulin resistance
- or a medication of steroids that you needed but has that unfortunate side effect.
So if there’s one takeaway from this section, it would be to ask your doctor to:
- Tell the difference between a temporary good A1C result and one that actually means there is no diabetes.
- And to tell me what would make you step in early before it gets out of hand.
Because the next question talks about how to screen even if the A1C looks normal so that you can catch things before they get out of control.
And unfortunately, a lot of people make this mistake.
Question 3: Do I still need screening if my score is great?
They feel absolutely phenomenal.
They feel better than they had in years.
And oh, you know, the A1C doesn’t show diabetes anymore, so that means they don’t have it anymore (Not true), so they just cancel their follow-up appointments.
- They don’t show up to the eye doctor like they’re supposed to.
- They don’t go to the foot doctor like they’re supposed to.
- They don’t follow up with the endocrinologist or their own PCP.
There was a patient that just showed up the other day at the clinic who we hadn’t seen in about a year and the A1C more than doubled.
Went from 7 to over 16.
And so if he had been doing his regular appointments and checkups, we could have caught that early and done something about it sooner rather than later so that the damage doesn’t accumulate during that time.
So, let’s take a moment to see what’s actually happening.
Because in the case of that patient, he got back an A1C that he was happy with.
He felt great. He had more energy.
And why would you prefer to go to the doctor’s office instead of enjoying your life?
It makes complete sense to:
- Spend time with family and friends
- Go out
- Enjoy a new restaurant without any worries
- Go to your kids’ game
- Take your significant other on a on a date night
There are a ton of other ways to spend your time having to budget a couple of hours to go see the doctor.
But here’s what needs to be understood:
A good A1C does NOT mean the diabetes is gone.
It just tells you that the fire is lower right now.
More importantly, a good A1C does not prove that the smoke damage was never there.
So, I’ll give you an example.
I was grilling burgers and hot dogs for Father’s Day recently, and it was raining that day.
So my dad brought the grill closer to the patio door.
That way, we can grill while inside the door and only get kind of sort of wet while flipping burgers.
Anyways, as you can imagine, there was a grease fire and the wind was blowing into the house.
So, all the smoke followed the wind into the house.
And if I hadn’t closed the grill cover to put out the flames, they might have come inside, too.
Afterwards, we enjoyed some well done burgers and hot dogs, but the whole place was smoky for a couple of hours and smelled like burnt meat.
Just a reminder to be careful next time if we decided to grill in that way again.
Same thing happens with diabetes.
The fire of the A1C might be out, but the smoke can linger in the air.
And if you didn’t know that the fire is out, you might think that a fire is already raging somewhere and you need to go find it to put it out.
So, the damage doesn’t start on the day your doctor says the word “diabetes.”
It started years ago when your blood sugar first began climbing quietly.
The potential for a grease fire goes up.
The smoke is already building and you won’t even know it.
There might not be any symptoms yet.
But once the fire appears, the diagnosis is made.
Diagnosis is just the moment someone finally checked.
So by the time that label gets attached,
- your eyes
- your kidneys
- your nerves
- your feet
They may have been living with elevated glucose for years.
And those changes can be completely silent with
- no symptoms,
- no warnings,
- just a quiet footprint that nobody looked for yet.
So that’s why we screen on a regular basis.
The fire may not be raging right now.
Your diabetes may not be loud right now, but we but we need to know what the earlier exposure already left behind.
So, if you think of it like smoke damage after the fire, the fire might be out and the house looks fine from the outside, but you still need an inspection to know what happened:
- To the walls
- To the wiring
- To the foundation
Because some damage only shows up when someone looks very closely.
So, how do we look closely?
Some questions you can bring to your doctor include:
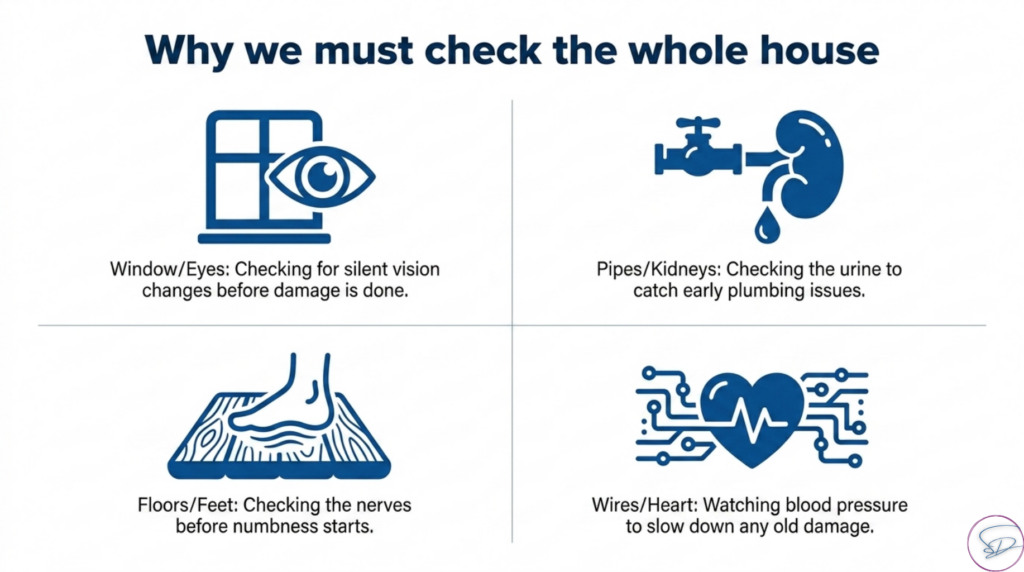
- Whether or not you need a dilated eye exam and how often.
- Diabetes shows up in the eye as retinopathy
- and it can be completely asymptomatic
- which means your vision can be completely normal… until it’s not.
- And when it’s not normal, the damage could already be done and it’s irreversible.
- You won’t feel anything in advance.
- So, we have to make sure that we take good care of our eyes in order to make sure that we catch any problems early before irreversible damage occurs.
- The next thing is: should we check our kidneys?
- We often need to check the albumin to creatinine ratio and the filtration rate of the kidneys.
- That’s how we catch early kidney damage before anyone feels that anything is wrong.
- We often need to check the albumin to creatinine ratio and the filtration rate of the kidneys.
- The other thing is that we need to check for neuropathy.
- So we need to get a foot exam and we do this because we want to check for nerve damage and foot problems that might be silent.
- There are some people that come in the door already alarmed by the numbness or the burning pain.
- At that point, we’re lucky enough to get that checked, but the damage has already happened.
- So, we want to make sure that we catch these canaries in a coal mine early enough to make a decision that can change the course of this outcome.
- So we need to get a foot exam and we do this because we want to check for nerve damage and foot problems that might be silent.
- And also we want to check blood pressure and cholesterol levels
- Because controlling these can slow down any existing damage any buildup of plaque in the arteries that can lead to heart attack or stroke.
So the main thing I hope you keep in mind is that these tests are not checking whether we can see the fire directly.
We are checking whether the years before your diagnosis already left a footprint.
We’re trying to figure out: Are we already behind.
And if something shows up after your A1C looks absolutely immaculate, that’s not a sign that your hard work hasn’t paid off.
It’s a sign that the injury started earlier than we realized and now you caught it in time to do something about it.
So remission can lower your future risk, but it cannot erase the period of exposure that came before it.
So congratulations!

I genuinely mean that.
You deserve the celebration because you did the hard work to earn it.
The next time you see someone post a dramatic A1C drop, celebrate them.
It truly is a job well done that deserves every bit of that recognition.
And now you know something that nobody else in that comment section knows,
which is to say that just because the fire is out doesn’t mean you can let your guard down.
You can rest while keeping your guard up.
So ask your provider these three main questions:
- Is this true remission or just improved control?
- Because the body will remember.
- How do we prevent relapse?
- Because relapse doesn’t announce itself. It creeps in quietly through the habits that were always serving you.
- And do I still need screening even though my A1C looks great?
- Because a good A1C tells you that the fire is lower, it doesn’t necessarily prove that the smoke damage was never there.
And this is how you keep your eyes open.
This is how you continue to look for the smoke.
You watch for signs that the fire might rekindle.
Just like how Smokey the Bear taught us how to prevent forest fires because if something does start to flare up again, you want to catch it before it gets out of control.
That’s what your doctor wishes you would ask.
If any of these questions hit close to home, please drop them in the comments.
Let’s have the conversation you wish you had with your doctor because that’s exactly why I’m here.
And and if this video helped you see your diabetes journey differently,
Please, it would mean the world to me if you share it with someone who needs to hear it.
Thank you so much for watching and listening.
Health and Wellness coaching
Would it be a bad idea to work together now?
If You’re Not Ready Yet, That’s OK.